Practice growth guide
How to Scale a Group Therapy Practice in Ontario
A practical framework for therapists building a group practice: systems, hiring, client acquisition, intake conversion, and how the owner role must change—without hype or empty motivation.
- Systems-first growth, not headcount for its own sake
- Marketing, intake, and operations treated as one pipeline
- Built for therapists and allied health clinic owners
- Ontario-based, virtual consulting across Canada
Quick answer
Scaling a group therapy practice is not simply hiring more clinicians. Sustainable scale requires a repeatable way to attract qualified leads, convert them through intake and consults, retain clients, and run scheduling and admin without the owner in every thread. When those pieces are weak, adding therapists usually adds chaos—not profit.
On this page you will see what “scaling” actually means, when you are (and are not) ready, a staged roadmap, the systems that should exist before aggressive hiring, and how marketing and intake work together.
What you will learn
- How growth differs from a scalable operating model
- Four practical stages from foundation to operational maturity
- Which systems matter before you hire
- Why intake often matters more than raw lead volume
- How the owner role must shift as the team grows
What scaling actually means
Growth can mean more revenue this quarter. Scale means you can add capacity (clinicians or sessions) without linear growth in your time, rework, and firefighting. Many practices grow revenue while the owner becomes more exhausted—that is growth without scale.
Common mistakes we see when practices try to “scale” too early:
- Hiring clinicians before intake, scheduling, and billing workflows are documented
- Relying on the owner's network as the only predictable lead source
- Weak or slow response to website inquiries and voicemail
- Generic positioning (“we see everyone”) that makes marketing and SEO expensive
- Adding modalities or populations before the core offer is full and referrable

When you are ready to scale—and when you are not
- Stable demand: waitlist or consistent inbound interest
- You can articulate niche, fees, and who you do not serve
- Basic CRM or tracking: you know where leads come from
- Scheduling and billing rarely fall through the cracks
- You are willing to delegate clinical matching and admin decisions
- Inquiries sit unanswered or bookings require multiple back-and-forths
- No clear consult process or inconsistent follow-up
- Revenue feels random month to month
- Owner is still the only person who can “fix” scheduling conflicts
- Hiring is meant to fix a positioning or demand problem
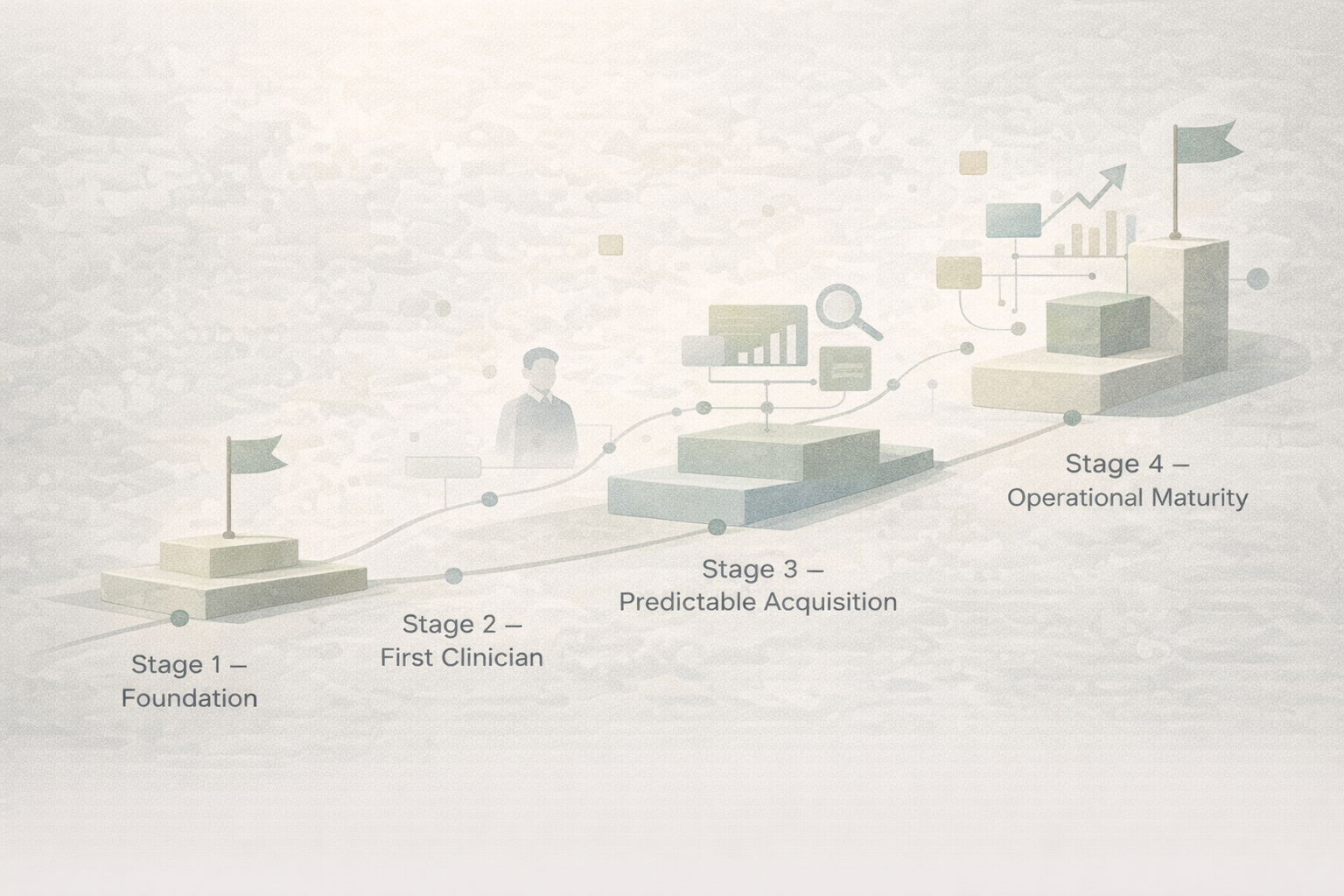
A staged roadmap
Use this as a sequence, not a checklist to rush. Each stage has one primary KPI so you know whether you are ready to move on.
Clarity and capacity to serve demand well.
- What to build:
- Ideal client, service menu, fees, policies, basic website, one primary booking path.
- Biggest mistake:
- Optimizing ads before the website and intake can convert.
- KPI that matters:
- Consult-to-booking rate; time-to-first-response on inquiries.
Replicate your standard of care without you in every session slot.
- What to build:
- Role descriptions, onboarding checklist, note and handoff norms, shared calendar rules.
- Biggest mistake:
- Hiring part-time without enough demand to protect their hours.
- KPI that matters:
- Clinician utilisation (sessions booked / available hours).
Steady flow of qualified leads and a tight path to first session.
- What to build:
- Service pages, local visibility, optional paid search, scripted consult flow, admin coverage.
- Biggest mistake:
- Buying leads when intake leaks (slow reply, no follow-up).
- KPI that matters:
- Cost per booked client (blended); lead-to-consult speed.
Decisions and exceptions flow through systems and leads, not only you.
- What to build:
- Weekly ops rhythm, simple dashboards, clear escalation rules, middle management or lead clinician.
- Biggest mistake:
- Adding locations or services while the core engine is still brittle.
- KPI that matters:
- Owner hours on admin; revenue per full-time equivalent clinician.
The systems you need before hiring aggressively
Hiring into a broken pipeline burns cash and morale. These systems are the minimum viable operating layer for most group practices we work with.
Intake workflow
Single inbox, assignment rules, SLAs for first reply, and clear handoff to scheduling.
Lead response speed
Target response within business hours; after-hours auto-reply with next steps.
Consult call process
Structured questions, fit criteria, fee conversation, and same-day booking offer when appropriate.
Scheduling and admin
One source of truth for calendars; cancellation and no-show policy applied consistently.
Clinician onboarding
First-week checklist: caseload expectations, documentation, supervision touchpoints.
Documentation and SOPs
Short Looms or written SOPs beat perfect policy manuals nobody reads.
Payroll and contractors
Clear splits, invoicing rhythm, and who owns receivables risk.
Reporting
Weekly snapshot: inquiries, consults held, new clients, utilisation, and no-shows.
Need help building intake and booking flows? See our intake system build and done-with-you consulting.
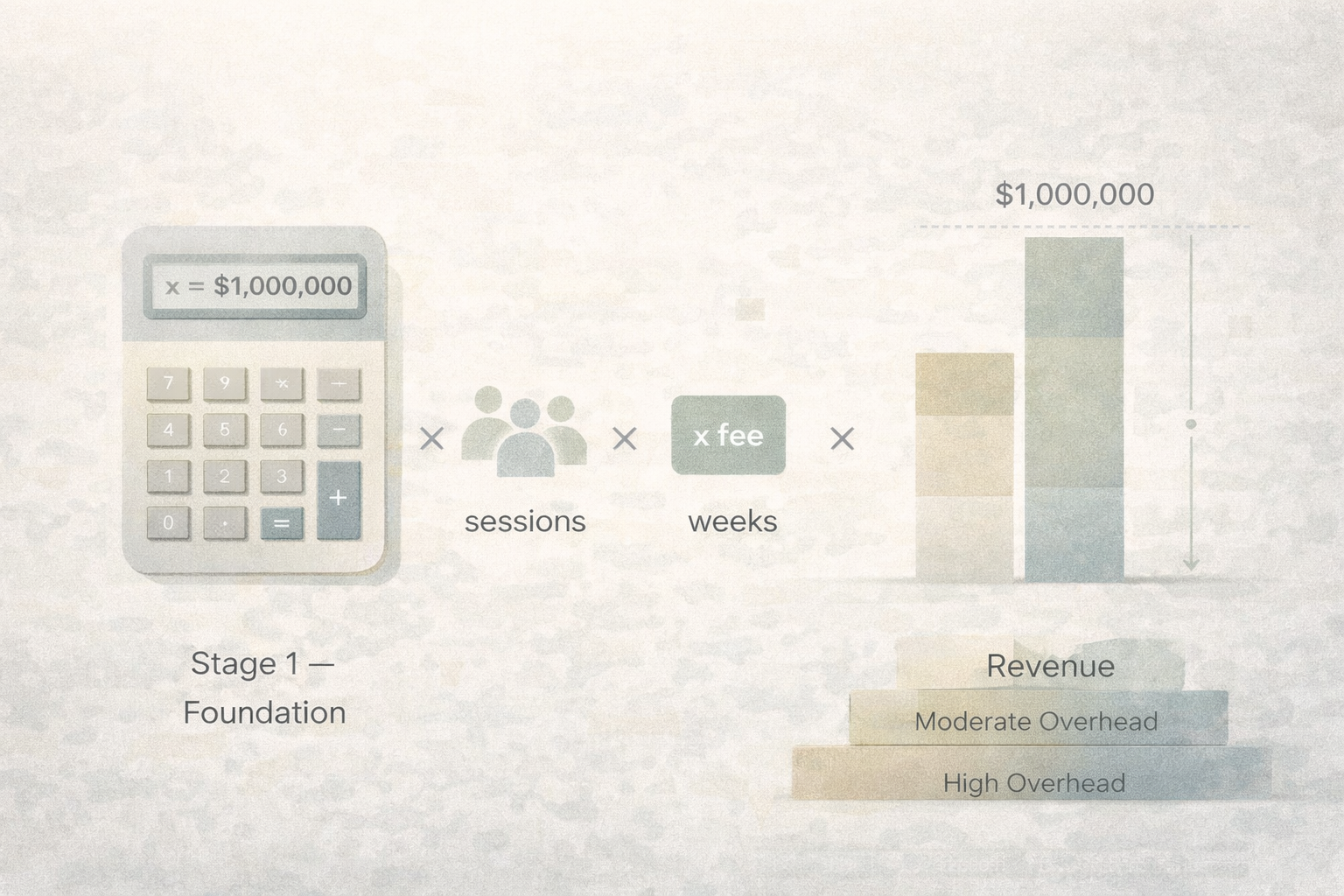
The simple math behind a seven-figure group practice
Seven figures in gross revenue is arithmetic, not magic. Illustrative example only—your fees, mix of services, and overhead will differ:
Assume 4–6 full-time equivalent clinicians, each averaging 22–26 billable hours per week, at roughly $150–$190 per session (CAD), 46 working weeks.
Rough order of magnitude: that band often lands in the high six figures to low seven figures in gross clinical revenue before overhead.
Revenue alone is not a healthy business. Margin, rent, software, marketing, admin payroll, and owner compensation matter. So does retention: high churn quietly destroys utilisation and referral momentum.
How to actually fill clinician calendars
1. Positioning and niche clarity
Specific service pages (“anxiety therapy for professionals,” “couples in crisis”) outperform generic homepages for search and ads. Align with what you can staff and deliver consistently.
2. Website conversion
One primary action per page, mobile-fast load times, fees or ranges where appropriate, and trust signals (approach, credentials, process). See website optimization.
3. Local SEO and search visibility
Google Business Profile, consistent NAP, and content that answers how clients search in your city. Our content and SEO work supports this when you are ready to invest consistently.
4. Paid ads, referrals, follow-up
Google Ads can work when intake is tight; referrers need simple pathways and occasional touchpoints. Always instrument follow-up on non-booked consults where ethics allow.
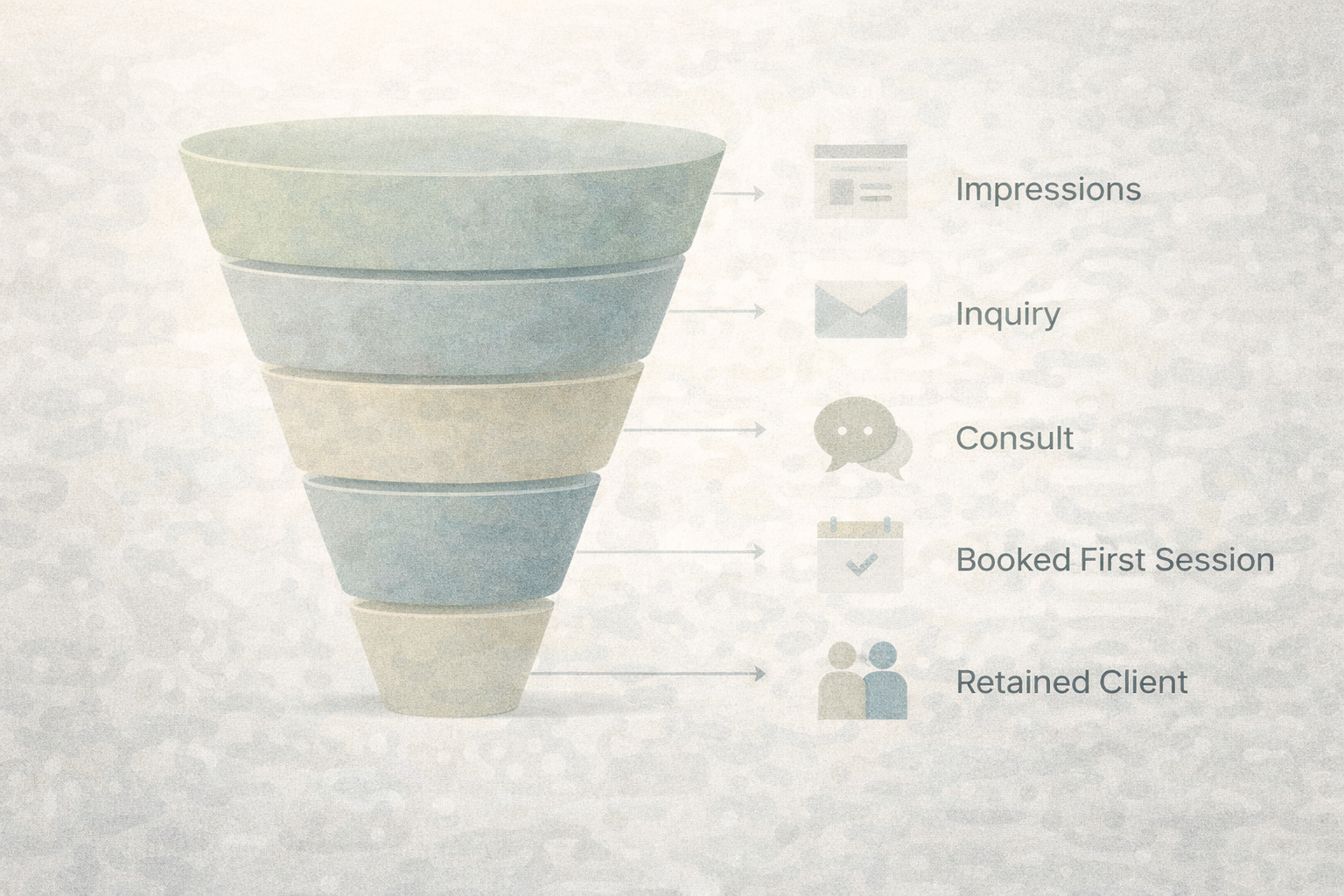
Why intake and consult conversion matter as much as marketing
Lead generation without conversion is expensive noise. Practices leak revenue in slow replies, vague consults, calendar friction, and unclear next steps after the call. Training a simple consult structure—fit, expectations, fees, booking—often raises yield without increasing ad spend.
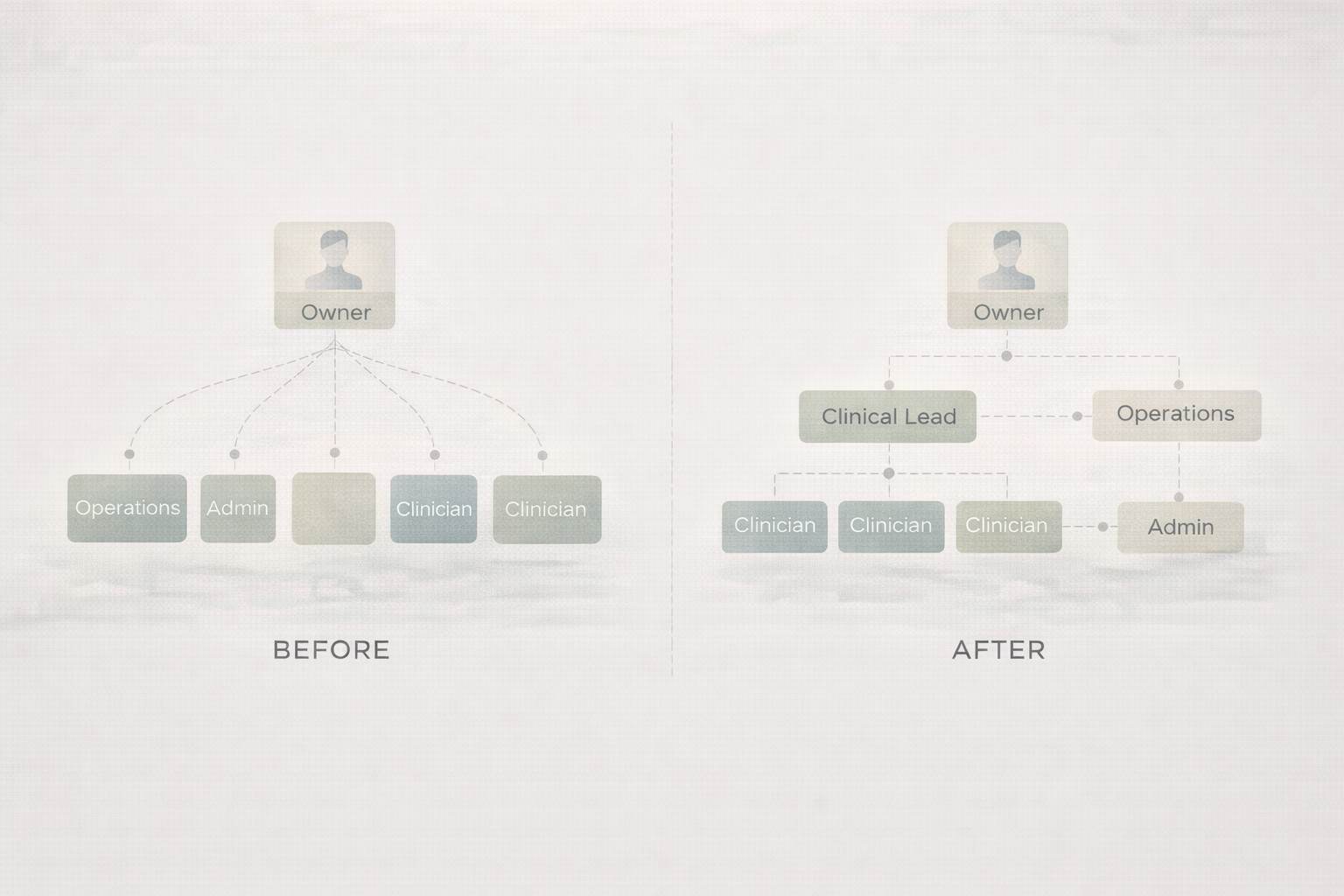
The owner role has to change
Beyond a certain size, the owner cannot be the primary clinical capacity and the only operator. Scaling requires delegation: clear scorecards (e.g. utilisation, consult conversion, wait time to first session), a weekly management rhythm, and explicit decision rights so bottlenecks surface early.
Common bottlenecks that keep practices stuck
How Allied Edge helps
We work with therapists and allied health clinic owners who want practical systems—not generic motivation. Typical engagements focus on client acquisition, intake and consult conversion, operational clarity, and the transition from solo provider to team-based growth.
- Therapy practice consulting for strategy, prioritization, and accountability
- Done-for-you services when you want implementation support
- Solo → group practice program when you are hiring your first clinicians
- Private therapy clients in Ontario — companion resource on acquisition fundamentals
This is for you if…
- You are moving from solo to a small group and want a sane sequence
- You have clinicians but lack a predictable growth and intake system
- You get leads but lose them between inquiry and first session
- You need operating structure before opening another location or service line
- You want sustainable growth without sacrificing clinical quality or ethics
Frequently asked questions
- How many therapists do I need to reach seven figures?
- There is no single number. Gross revenue depends on fees, utilisation, weeks worked, and mix of services. Many practices approach seven figures in clinical gross with roughly four to six full-time equivalent clinicians at common Canadian fee bands—but overhead and owner pay determine whether that is actually a strong business.
- Should I hire before I have a waitlist?
- You need predictable demand or a clear plan to generate it. A waitlist is one signal; consistent inbound inquiries and consults are another. Hiring without a pipeline often leads to underutilised clinicians and cash-flow stress.
- What systems should a group practice have before scaling?
- At minimum: intake and response standards, a documented consult flow, scheduling rules, onboarding for new clinicians, and a weekly metrics snapshot. Add formal admin roles when owner time on logistics crowds out leadership.
- Is SEO or Google Ads better for therapy practices?
- Neither is universally better. SEO and content compound over time; ads can fill capacity faster when landing pages and intake are strong. Many mature practices use both with clear tracking.
- How long does it take to scale a group practice?
- Foundations often take a few months; predictable acquisition and full team utilisation commonly unfold over one to three years depending on market, positioning, and execution—not promises, just typical ranges we observe.
- Can a therapy practice scale without multiple locations?
- Yes. Virtual care, extended hours, and a larger clinical team can grow capacity within a single physical footprint. Second locations add complexity; they rarely fix a weak core operating model.
- What is the biggest bottleneck in group practice growth?
- Frequently intake: slow response, unclear consults, and booking friction. Marketing bottlenecks matter too, but we see more practices underinvest in conversion than in attention.
- What metrics should I track in a therapy group practice?
- Inquiries, consults held, new clients, clinician utilisation, average wait time to first session, no-show rate, and revenue per clinician. Keep the dashboard small enough to review weekly.
- What should a consult call process include?
- Clarify presenting concerns and goals, explain fit and approach, discuss fees and policies, answer questions, and, when appropriate, offer specific appointment times before ending the call.
- When should I hire admin support?
- When delayed follow-ups are costing bookings, or when owner and clinicians spend meaningful weekly time on scheduling that could be systematised or delegated. Earlier admin is often cheaper than lost clients.
Build a stronger group practice—not just a bigger one
If you want an outside perspective on systems, intake, and growth sequencing, start with a conversation. No pressure, no jargon—just clarity on next steps.